Let's be real. Searching for the "best treatment for menopause" feels like looking for a magic bullet. You're hit with hot flashes that make you want to stand in a freezer, nights spent wrestling with sheets instead of sleeping, and maybe a mood that swings like a pendulum. You want it to stop. Now. The truth you might not find on a quick Google search? There is no single "best" treatment. What works wonders for your friend might do nothing for you, or worse, cause side effects you don't want. The real answer lies in a personalized strategy, a plan built around your unique symptoms, your health history, and your personal preferences.
Think of it less like picking a pill off a shelf and more like designing a custom toolkit. Your toolkit might include prescription hormones, other medications, specific supplements, targeted lifestyle tweaks, or a combination. The goal isn't just to survive menopause, but to thrive during it. This guide will walk you through how to build that toolkit, step by step.
What You'll Find in This Guide
Understanding the Menopause Transition (It's a Process)
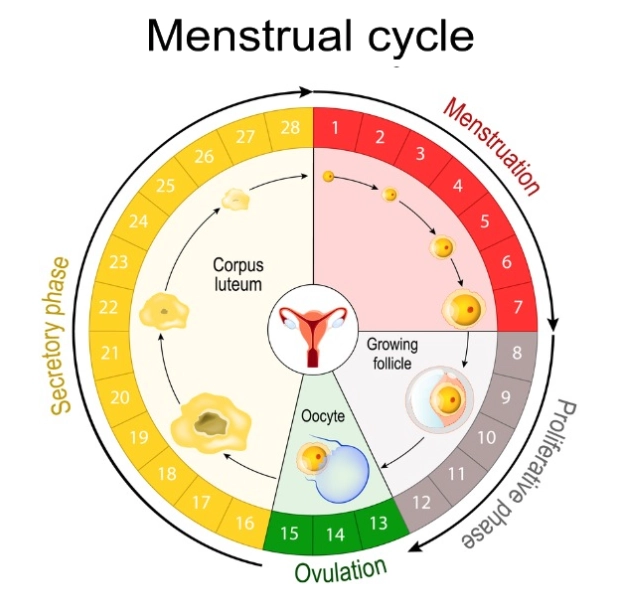
Many women are surprised to learn menopause is a point in time, not a condition. It's officially diagnosed after you've gone 12 consecutive months without a menstrual period. Everything leading up to that point, and everything after, has its own name and character.
Perimenopause: The Lead-Up
This is the phase where most of the action—and the misery—happens. It can start 8-10 years before menopause. Your ovaries begin their erratic wind-down, causing wild fluctuations in estrogen and progesterone. This is when symptoms like irregular periods, hot flashes, sleep problems, and brain fog often debut. It's chaotic, unpredictable, and frankly, exhausting.
Postmenopause: Life After the Change
Once you're 12 months period-free, you're postmenopausal. Your hormone levels settle at a new, low baseline. While acute symptoms like hot flashes often ease over time (though they can persist for some), the long-term effects of low estrogen become the focus: things like vaginal dryness, increased risk for osteoporosis, and changes in heart health. Treatment in this phase often shifts toward managing these chronic aspects.
Step 1: Honestly Assess Your Symptoms
Before you can choose a path, you need a map of your own terrain. Grab a notebook or your phone and track for a week or two. Don't just note "had a hot flash." Get specific.
Vasomotor Symptoms (The Heat Wave): How many hot flashes/night sweats per day? Are they mild (a warm flush) or severe (drenching sweat)? Do they wake you up 3 times a night?
Genitourinary Syndrome (GSM): This is the clunky medical term for vaginal dryness, pain during sex, urinary urgency, or recurrent UTIs. It's incredibly common and often underreported because women don't connect it to menopause.
Sleep & Mood: Are you lying awake or waking up constantly? Is your mood low, anxious, or irritable in a way that's new for you?
Other Players: Brain fog, joint aches, hair thinning, weight gain around the middle.
I've worked with women who downplayed their 5-6 daily severe hot flashes as "just something to deal with," while others sought help for mild but annoying warmth. There's no right or wrong level of bother—it's your life. But being precise helps your doctor—and you—understand the target.
Hormone Therapy: A Deep Dive on the Most Effective Option
For moderate to severe vasomotor symptoms and GSM, estrogen-based hormone therapy (HT or HRT) is the most effective treatment we have. It's not a debate; it's what decades of clinical evidence show. But the devil—and the success—is in the details: the type, dose, route, and duration.
One major misconception I see? Women think HRT means one specific pill. It's a whole category.
| Type of HRT | What's In It | Who It's For | Delivery Examples |
|---|---|---|---|
| Estrogen-Only Therapy (ET) | Just estrogen. | Women who have had a hysterectomy (uterus removed). Adding progesterone isn't needed to protect the uterus. | Patches (Climara, Estradot), gels (EstroGel), sprays, pills. |
| Combined Estrogen-Progestogen Therapy (EPT) | Estrogen + a progestogen (synthetic progesterone) or progesterone (body-identical). | Women with a uterus. The progestogen protects the uterine lining from the cancer risk posed by estrogen alone. | Combined patches (Combipatch), pills, or separate prescriptions (e.g., an estrogen patch + oral micronized progesterone). |
| Low-Dose Vaginal Estrogen | Very low-dose estrogen applied locally. | Primarily for GSM symptoms (dryness, pain). Minimally absorbed, so it's safe for most women, even many with a history of breast cancer. | Creams (Estrace), tablets (Vagifem), rings (Estring). |
The Route Matters More Than You Think
This is an expert nuance many miss. Transdermal estrogen (patches, gels) is absorbed through the skin and bypasses the liver. This means a lower risk of blood clots and less impact on triglycerides compared to oral estrogen pills. For many women, especially those over 60 or with risk factors for blood clots, patches/gels are the smarter first choice.
Body-identical progesterone (micronized progesterone, brand name Prometrium) is generally preferred over synthetic progestins for its better side effect profile (less bloating, breast tenderness) and possibly a better risk profile regarding breast cancer when used with estrogen, as noted in studies like the KEEPS trial.
The golden rule? Start low, go slow. Begin with the lowest dose that might work. You can always nudge it up in 3 months if needed. Starting with a high dose often leads to side effects (breast tenderness, bloating) that make women quit prematurely.
What If Hormones Aren't For You? Exploring Non-Hormonal Paths
Not everyone can or wants to use hormone therapy. Maybe you have a personal history of hormone-sensitive cancer, a strong family history that gives you pause, or you simply prefer to avoid hormones. Your toolkit is still full of options.
Non-Hormonal Prescription Medications: These are powerful tools often overlooked.
- SSRIs/SNRIs: Antidepressants like paroxetine (Brisdelle, a low-dose version approved for hot flashes), venlafaxine, or escitalopram can reduce hot flash frequency by 50-60%.
- Gabapentin: An anti-seizure drug that's very effective for night sweats and sleep-disrupting hot flashes.
- Clonidine: A blood pressure medication with a side effect of reducing hot flashes.
These don't help vaginal dryness or protect bones like estrogen does, but for pure heat relief, they work.
Vaginal Moisturizers & Lubricants: For GSM, non-hormonal options are essential. Daily moisturizers (like Replens) help maintain baseline tissue health. Water- or silicone-based lubricants (like Uberlube, Sliquid) are a must for comfort during sex. Don't suffer in silence here—these are game-changers.
Lifestyle & Behavioral Strategies (The Foundation): These aren't just fluff. They're the bedrock that makes any other treatment work better.
- Layer Your Clothing: Sounds simple, but cotton layers you can peel off are a frontline defense.
- Cool Your Sleep Space: A bedroom at 65°F (18°C), moisture-wicking pajamas (like bamboo), and a cooling pillow pad.
- Mindful Breathing (Paced Respiration): When you feel a hot flash start, practice slow, deep belly breathing. Studies show it can reduce severity.
- Regular Exercise: Aim for 150 minutes a week of moderate activity. It helps regulate mood, sleep, and weight, and may modestly reduce flashes.
- Watch Triggers: Spicy food, alcohol, caffeine, and stress are common hot flash instigators. A food diary can help you spot yours.

How to Talk to Your Doctor About Menopause Treatment
This is where the plan becomes real. Many doctors are still catching up on modern menopause management. Be prepared to lead the conversation.
1. Bring Your Notes: Walk in with your symptom log. "Doctor, I'm having about 8 severe hot flashes daily and they wake me up 3 times a night. It's affecting my work and mood." That's powerful.
2. State Your Goal: "I'd like to discuss options to manage these symptoms so I can sleep and function better."
3. Ask Specific Questions:
- "Based on my age and health history, am I a candidate for hormone therapy?"
- "If so, would a transdermal estrogen patch and body-identical progesterone be appropriate for me?"
- "If not, can we discuss non-hormonal options like gabapentin or an SSRI?"
- "What is our plan for reviewing this treatment in 3 months?"
4. Discuss Your Health Context: Be ready to talk about your blood pressure, cholesterol, family history of breast cancer/heart disease/osteoporosis, smoking status, and personal history of blood clots. This info is critical for safe decision-making.
If your doctor dismisses you or seems unwilling to discuss these options in depth, consider finding a menopause specialist. Organizations like the North American Menopause Society (NAMS) have a directory of certified practitioners.
The journey through menopause is deeply personal. The "best treatment" is the one that safely and effectively gives you back your comfort, your sleep, and your sense of control. It's the strategy you and a knowledgeable healthcare provider build together, piece by piece, based on the evidence and your lived experience. Start the conversation. You deserve to feel better.




Leave a comment